Download a PDF of the Get Loud Louisiana Ending the Epidemic Plan by clicking the cover below, to read it online, scroll down to the chapter index located here.

Ending the Epidemic Plan 2021 – 2025
Introduction
Louisiana has a deep history and unique culture formed over centuries, marked by trauma stemming from causes such as too many devastating hurricanes (including several during the writing of this plan) and systemic racism dating back to our beginnings during the Trans-Atlantic Slave Trade. !at same history has also made Louisiana a beautiful melting pot of Black, French, Spanish, Haitian, African, and Indigenous people that has given rise to Creole and Cajun cultures, including our own languages and cuisine. That history has also birthed musical genres and styles of dance from Jazz to Bounce and Zydeco, Second Lines and Mardi Gras Krewes, and so much more.
Today, Louisiana is known for many things —its food, music, and football, to name a few. But most of all, it’s the people that make Louisiana so special. It is perhaps because of the unique shared adversity that comes with living in a place like this, namely the frequency of storms and the impacts they have on our homes, health, and livelihoods, that Louisianans are the type of people who will always help a neighbor in need and who are always ready to celebrate life together.
This plan was written with these people —our communities—in mind, and with our history and the unique landscape in which we live guiding our strategy. Louisiana has made some major progress over the past several years when it comes to HIV. Last year, the Office of Public Health announced that the number of people newly diagnosed with HIV in Louisiana had declined over 20% in the past four years from 1,124 new cases in 2016 to 989 in 2018, and 891 in 2019. 2018 was the first year since 2005 that there have been fewer than 1,000 new HIV diagnoses, and the downward trend we saw in 2019 has brought us to the lowest number of new diagnoses since the epidemic began in the 1980s. However, we still have a lot of work to do in order to meet 2030 targets. According to the CDC, Louisiana ranked 4th in the nation for HIV case rates in that same year. Stigma and misinformation still work to slow our progress, as do difficulties in accessing testing and treatment services.
The five-year plan laid out across the following pages reflects the collaboration of so many individuals, community-based organizations, and a variety of stakeholders from around the state. We will take you through our guiding principles, our overarching goals, the process that brought us to this point, and how you can join the movement and Get Loud too. We will then outline our objectives and strategies in five focus areas, highlighting the amazing work and experiences of people living with HIV (PLWH), healthcare workers, and advocates doing the work across Louisiana along the way.
Get Ready to Get Loud!
Many community leaders across the United States are calling for an end to the HIV epidemic in their cities, their counties, and their states through the development of Ending the Epidemic (EtE) plans. We now have the tools to effectively do just that— from PrEP (Pre-Exposure Prophylaxis) which allows people to remain HIV-negative and much improved medications that allow PLWH to enjoy the same life expectancy as people without, to proof that Undetectable=Untransmi”able (U=U) allows PLWH to prevent the transmission of HIV to intimate partners. We are in a position to create ambitious and bold plans to improve health outcomes for all people living with and vulnerable to HIV, reducing its impact and bringing new infections below epidemic levels.
As of June 30, 2020, a total of 22,401 persons were living with HIV in Louisiana; of these individuals, 11,217 persons (50%) have an AIDS diagnosis. In 2018, Louisiana ranked 4th in the nation for HIV and AIDS case rates (21.2 per 100,000 and 9.1 per 100,000 population, respectively) and 11th and 12th in the number of estimated HIV and AIDS cases, respectively. Rates of other sexually transmi”ed infections (STIs) also remain high in Louisiana. In 2018, Louisiana ranked 2nd in chlamydia case rates, 5th for gonorrhea, and 7th for syphilis. While estimating the number of people living with Hepatitis C (Hep C) is a challenge due to historically low rates of testing, our data suggest that at the end of 2019, there were 63,450 people in Louisiana living with chronic Hep C.
We thought a lot about what we want this plan to accomplish and about what ties us together. First, we see this as an opportunity to do something different! We want to step out of the box to create something truly bold and innovative. We want to start talking more about HIV, STIs, Hep C, and sexual health. We want to break down the stigma and misconceptions that surround HIV, Hep C and STIs. We want to li% up the voices of those who are living with HIV and those who are impacted—and make sure
they are the ones leading the way forward.
Second, we thought about what brings us together as a state—and what do Louisianans love more than anything (except maybe Maw-maw’s gumbo)? MUSIC. Whether it’s Jazz, Bounce, Zydeco, Blues, or Country: when it starts playing, we can’t help but get up and move! !at is the kind of excitement we want to bring to this plan and to the work. We want to bring people in, demonstrate what we all have in common, celebrate what makes us different, and work together to find solutions so that we can all lead healthy, full lives. We aren’t going to end the epidemics unless we do it together.
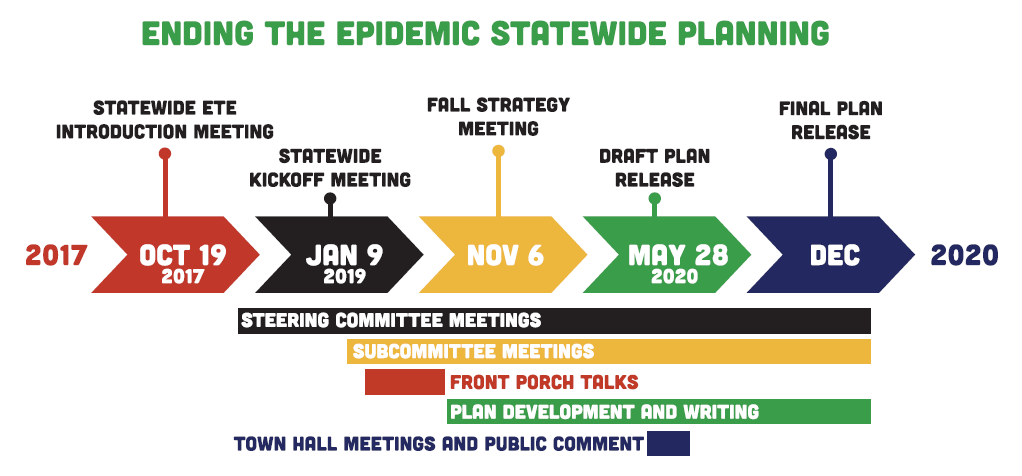
Public health practitioners and community advocates began conversations of taking on an Ending the Epidemic Plan in Louisiana in late 2017. However, when the decision was made to embark on the development of an EtE plan, the Louisiana Department of Health wanted to be intentional about meaningful involvement of the community, particularly PLWH. They began a search for a community-based organization to lead the charge. About one year later, in 2018, they enlisted the help of Women With A Vision, a social justice organization with roots in the early days of the HIV Epidemic and 30 years of history working with communities of color and marginalized populations, to gather community input and ensure a community-driven process.
The process was reinvigorated when 70 providers, community members, advocates, and public health workers from around the state came together again at a statewide meeting
in Lafayette in January 2019 to identify barriers, priorities, and solutions for how to improve the lives of those living with, and impacted by, HIV and how to End the HIV Epidemic in Louisiana.
Between March and July 2019, the team traveled across the state holding a series of community conversations, or Front Porch Talks, with 15 groups in six cities, including Baton Rouge, New Orleans, Lafayette, Lake Charles, Monroe, and Shreveport, to gather feedback to inform the statewide EtE plan – and to recruit community members to engage at all levels of the planning process, by joining subcommittees focused on our five priority areas, as well as our coordinating bodies, the Steering Committee and Core Team.
Key themes arising from the Front Porch Talks would form the backbone of our plan and can be seen throughout our plan. Examples include a need for community education around HIV and safer sex practices, improved transportation services, stable housing, more holistic approaches to care, be”er availability of information on where to access care and other resources such as mental health care and substance use supports. Stories of stigma and discrimination were widespread, including in medical se”ings, and reinforced our need to focus our sights on stigma reduction before all else.
The team then entered a stage of synthesizing feedback from community meetings and committee meetings to begin drafting the goals, strategies, and activities that would become our Statewide EtE Plan. A second statewide meeting was held in November 2019 to bring participating members back together to spend time developing our objectives in workgroups.
Throughout 2020, subcommittees met to continue drafting strategies and activities for both a detailed work plan and the community plan you are reading today. Working during the COVID-19 Pandemic certainly changed the course of the work in many ways. Our team had intended to revisit the groups we met with during our Front Porch Talks to provide updates, and planned for five in-person town hall meetings around the state to share our work with new stakeholders.
Instead we offered virtual community conversations to debrief around how COVID-19 was impacting our communities and held two virtual town halls and an online public comment period in the Spring of 2020 to share our dra% plan with a broader audience and to give community members the opportunity to let us know if we were still on the right track. With positive feedback, we moved forward to refine both our community-facing plan and a detailed work plan that will be used to guide our way as we move into our implementation and monitoring and evaluation phases.
Ending the HIV epidemic in Louisiana is less about ending HIV than it is about addressing the intersections and social determinants of health which drive the epidemic. Today, HIV is a manageable chronic condition and those taking effective treatment live long, healthy lives. Additionally, people living with HIV who have a viral load of 200 or less have no risk of sexually transmitting HIV to a partner.
Working to end the HIV epidemic means working with advocates and communities across Louisiana to address racism, poverty, homophobia, transphobia, sexism, ageism, education reform, policing and criminalization, reproductive justice, immigration reform, HIV criminalization, and so much more. Each of these areas serve as drivers of the epidemic by oppressing communities, entrenching systemic inequities, furthering stigma, and, ultimately, embedding barriers which prevent people from accessing HIV prevention and treatment services. Addressing each of these drivers of the HIV epidemic will allow for a reduction in the number of new HIV diagnoses by expanding opportunities for all people to access critical prevention, treatment, and social services.
We have the tools to end the HIV epidemic and whether HIV advocacy has been your life’s work, or you have never even considered how HIV impacts your community, WE NEED YOU! !e time to end the HIV epidemic is now, but we must be intentional about creating mechanisms to coordinate, collaborate, and work across intersectional movements. Our ability to succeed in ending the HIV epidemic is fundamentally linked to the establishment of equity across the various systems and structures that are currently driving the epidemic.
This is a call to action to further align our efforts with other movements and an invitation to build coalitions in the following ways:
Anti-Racism:
We know that systemic racism has long impacted access to opportunity, financial stability, and quality healthcare. We must address the varied impacts of racism by bringing equity to educational institutions and employment practices both within the field of HIV and beyond. We must demand that our public health leadership, healthcare and service providers work to examine health disparities and overcome biases that negatively impact people of color; and we must hold partners who fail to work toward anti-racism accountable for those failures.
Economic and Housing Justice:
Financial security and stable housing are necessary to provide the security from which a person can take care of their essential needs, including their healthcare. Access to housing and living wages reduce behaviors that put people at risk of acquiring communicable infections, of experiencing violence and poor health outcomes. We believe that housing is prevention, and will stand with those fighting for economic justice and housing the houseless to help our communities achieve that security and wellbeing.
Anti-Transphobia and Homophobia:
Stigma and discrimination based on gender identity and sexual orientation are still pervasive in our country. In Louisiana, LGBTQ+ persons are still not protected against discrimination under the law. Trans women of color continue to experience disproportionate rates of violence against them, including homicide, compared to other groups2. We must work in tandem with advocates in the LGBTQ+ movements to continue to demand equality and to create trans- and queer-inclusive spaces within the organizations in which we work, the communities in which we live, and the services which we provide.
Anti-Sexism and Toxic Masculinity:
We understand that power dynamics and gender-based expectations rooted in our patriarchal system still create challenges for women trying to advance in their education and careers, result in their making 81 cents to every man’s dollar3, and leave them more vulnerable to sexual abuse, harassment, and intimate partner violence. Expectations of masculinity also lead to participation in violence, reduced likelihood to utilize mental health services, and higher rates of suicide among men. We will stand with partners and policymakers to create balance, close to gender pay gap, and dismantle toxic masculinity.
Reproductive Justice:
We stand with the Reproductive Justice Movement, as ours is inextricably linked. We know that the right to bodily autonomy, to decide when and if to have a family, and the ability to raise your family in a safe environment intersects with all other aspects of our lives. Reproductive Justice is about access to contraception, STI testing and treatment, and comprehensive sex education. It is about the ability to make a living wage, to afford and access childcare and the creation of spaces that support parents and families, and so much more.
Policing and Criminalization Reform:
The policing of poor people and communities of color has long factored into economic and health disparities. The criminalization of drug use, sex work, and disproportionate incarceration of and police violence against Black people has devastating, generational impacts on communities. Louisiana has, for many years, held the title for highest rates of incarceration in our country, making this commitment to work with advocates and activists calling to rebuild our justice and policing systems that much more important.
An End to HIV Criminalization:
The criminalization of HIV and other health statuses leads to further stigmatization of HIV and is antithetical to both the science of transmission as well as to the promotion of testing or status disclosure. It has detrimental impacts on prevention, health outcomes for people living with HIV, and is weaponized against people living with HIV to deliver harsher sentences for unrelated crimes. We must work in coalition to stop the criminalization of HIV to allow people living with HIV to do so without fear of persecution and as a key step to ending the epidemic.
In addition, we will stand with those fighting for more just immigration reform and education reform that be#er prepares our youth for the future, those fighting ageism and working for the security and dignity for our aging population, those continuing the hard-fought ba#le against ableism, and all those working to gain and preserve human rights in their myriad ways.
With the prevention and treatment options we have today, new HIV diagnoses and HIV-related deaths could both be rare. What continues to propel HIV to epidemic levels is how each of the factors laid out above have worked together to create the inequities inherently responsible for preventing people from accessing critical services. In that vein, we must strive to act together and across movements to end systems of oppression which have resulted in the health inequities and disparities that are so apparent in the HIV landscape.
Community-Driven
We want to make sure that we are not just consulting community members, but that community members are engaged at all levels of the process and that their needs and priorities guide our way.
People Living With HIV-Centered
We believe that people living with HIV, and other lived experiences, are the experts here and we want to make sure once again that theirs are the needs and priorities that come first.
Intersectional
We know many people face multiple barriers and systemic oppressions including racial and economic injustice, criminalization, housing insecurity, and stigmatization that impact their well-being, and as such, we will formulate our response to HIV in Louisiana through the intersections of these experiences.
Stigma Free
One of our primary goals is to end the stigma that surrounds HIV, sexual behavior, sexually transmitted infections, drug use, sexuality and gender. We want to break down stigma and misinformation, while lifting up the realities of what it means to live with HIV, including important truths such as U=U. Stigma and discrimination have no place in our plan or planning process!
Racial Justice
As outlined in the 2017 A Declaration of Liberation: Building a Racially Just and Strategic Domestic HIV Movement by the Racial Justice Framework Group8, a Racial Justice Lens for the HIV movement demands that we:
- Integrate racial justice into our organizations and political strategies;
- Center those communities most impacted by the epidemic in leadership and decision-making;
- Root our efforts to advance a racial justice lens in the HIV movement in accountability to the communities that we lead;
- Ensure equity around allocation of resources — human, material, and financial; and
- Work to transform and, where necessary, dismantle institutions that uphold white supremacy and compromise the wellbeing of communities of color.
Human Rights
Our work is guided by the following core Human Rights Principles developed by the United States Human Rights Network:
- Human Rights are universal, interdependent, indivisible, and inalienable;
- Human Rights movements must be led by those most directly affected by human rights violations;
- Human Rights advocacy and organizing should prioritize the struggles of the poor and most marginalized groups in society;
- Human Rights movements must be inclusive and respect and reflect the diversity within communities; and
- Human Rights encompass civil, political, economic, social, cultural, environmental, sexual, and development rights for individuals, peoples, and groups.
Get Loud! Committees
- Community Building with PLWH and Allies
- Prevention Education and Stigma
- Access to Care and Supportive Services
- Smaller Cities and Rural Communities
- Data Driven Policy and Advocacy
How are we getting loud?![]()
One of the goals of Get Loud Louisiana is to strengthen our community and lift our voices, together. We want to live in a Louisiana where all people—regardless
of who they are, where they live, who they love, or their health status —feel supported and heard. We want to see PLWH leading the charge when it comes to creating supportive spaces and advocating for their health and human rights.
We believe it is the work of allies to provide technical assistance, fundraising support, whatever is asked of them to support the needs, activities, and wishes of those with lived experience.
Measure and reduce stigma across Louisiana
- Reduce HIV-related stigma in our communities, as well as overlapping stigmas around sexual orientation, gender identity, class, race, and drug use
- Create community education and stigma-reduction campaigns based on results from surveys such as the Stigma Index Project
Create a network of People Living With HIV to lead social support and advocacy efforts across the state
- Build a network of Peer-Led support groups in every region of the state
- Identify, train and connect peer leaders
- Create paid opportunities for PLWH
- Connect network online and in-person
Build a network of trained advocates to lead efforts to improve the lives of PLWH and to reduce transmission
- Strengthen existing networks like Louisiana AIDS Advocacy Network
- Get community members involved in local politics and annual Legislative Awareness Days
Mobilize allies across the state to support advocacy and stigma reduction
- Work with community partners from a variety of sectors to support our causes and to educate their communities about HIV
- Train and engage allies in both formal and casual social se”ings to ensure they have clear understanding of what it means to be an ally – including using non-stigmatizing, person first language, understanding of intersectionality and the many ways we are impacted by our status, race, gender, class, and identity, and that they know how to operate on our behalf when needed
How are we getting loud?
Throughout the process of gathering input to create this plan, no matter who we talked to, three things were clear: we need to do a lot more to educate our communities and service providers, reduce stigma, and prevent new cases of HIV. !e more education and knowledge we share about HIV and how it is transmitted, the more we begin to chip away at the
stigma and fear that many people have around getting tested or sharing their status—and the more likely people are to engage in safer sex and drug use practices that reduce their risk.
We want to make sure that everyone knows about PrEP and where to access it, that condoms are commonplace, that U=U is a message heard in every home, and that PLWH are truly prevention warriors! !e more we talk about HIV, healthy sexual and drug use behaviors, the more comfortable people will feel Getting LOUD about getting tested, knowing their status, as well as what it means to live a healthy life while positive. By 2025, we want to significantly decrease the number of people without reliable access to
Prevention, Treatment, and Supportive Services. Here’s how:
Increase access to PrEP for all those who want it and would benefit from it
- Increase the number of providers who prescribe and manage PrEP
- Increase use of TelePrEP, particularly amongst priority populations with lower rates of use such as women, people of color, and members of the LGBTQ+ community
- Conduct public health campaigns and events that focus on diverse communities within our state
Increase the number of people who know their HIV status!
- Make testing for HIV, STIs and Hep C normal and routine
- Provide routine tests at annual checkups, ER visits, and all healthcare facilities
- Increase use of mobile testing units, telehealth, in-home testing, and testing at community-based sites (for example, churches, barber shops, salons, community centers, health fairs, and college campuses)
- Make sure everyone who is sexually active has had AT LEAST one HIV test in their life
- Raise awareness about testing availability, treatment options, and what it means to live positive
- Expand opt-out testing and access to prevention tools (condoms, PrEP, etc.) within prison and jail systems
Increase community-based and street outreach in both city centers and rural areas
- Create positions for Community Health Workers (CHWs) in all regions of the state to provide outreach services
- Recruit and train individuals from the communities most impacted by HIV to become CHWs and peer educators
- Increase participation in community events (education sessions, home health parties, health fairs)
- Provide outreach and education in community-based sites (such as barbershops, beauty salons, community centers, bars, shopping areas, faith-based organizations, HBCUs) as well as virtually
- Create and support community advisory boards in all nine public health regions of the state to ensure local leadership from communities most impacted by HIV, STIs, and Hep C
Increase access to sex education for our young people
- Increase partnerships between School Districts/Charter Systems and community partners to provide age-appropriate sex education to Louisiana students
- Survey parent attitudes on sex education
- Share HIV/STI rates among adolescents and adults to local authorities and school leadership
- Develop online sex education tools
- Train parents on how to provide sex education in the home through online tools and curriculum
- Advocate for updated legislation requiring medically accurate, age-appropriate, inclusive sex education be provided in public and charter schools, and allowing school-based surveys such as the YRBSS to ask our youth about risk-related behavior
Ensure people who inject drugs have access to sterile injection equipment and harm reduction services
- Ensure statewide access to Syringe Services Programs (SSP)
(harm reduction supplies and needle availability) - Expand mobile SSPs with outreach to rural areas
- Eliminate stigma around SSPs and people who use drugs
- Include safer sex and drug use information with outreach and services
Increase the diversity of the healthcare workforce to reflect those most impacted by the epidemics
- Create partnerships with HBCUs and universities/programs that have a high percentage of students of color to link to internship and work training opportunities
- Expand implementation of training programs for Black, Latinx, gay, trans, queer people to enter the HIV/healthcare workforce
- Create HR policies that value experience in hiring and promotion—placing value on lived experiences including, but not limited to experience with communities of color, the justice system, homelessness, drug use, alongside education and/or work experience
How are we Getting Loud?
Our goal is to make it easier for people across Louisiana to get into care, stay in care, and stay healthy. To us, this doesn’t mean just making sure that people are staying on their medication. It means having access to client-centered treatment and providers that clients feel comfortable with, not only for HIV services, but also for achieving optimal whole-person health. We recognize the many barriers people face when it comes to their health care, and we want to work with our community to meet them where they are, and to find solutions to overcome those barriers together. We will work with providers and community-based organizations to:
- Promote person-centered services
- Expand treatment options that work for clients no ma”er where they live and what modes of transportation they have access to
- Establish standards for clinics that provide accommodations for people who are not able access services during traditional clinic hours, or who might need support with childcare or the ability to bring their children with them to their appointments
- Work to create inclusive spaces where all are welcome regardless of gender expression, sexual orientation, housing status, employment status, drug use, language spoken, or immigration status
Ensure that clients living with HIV are assessed for and linked to psychosocial/supportive service needs (including mental health, housing, transportation, dental and vision care) within 14 days of diagnosis, and that they are rescreened at least annually
- Establish minimum standards and recommendations to ensure all facilities are adequately screening
- Streamline referral systems between HIV service agencies and mental health, dental, and vision care providers
- Expand use of peer support for newly diagnosed persons experiencing long wait times for certain types of services or who in need of additional support
- Strengthen mental health workforce at HIV service agencies and expand access to telemedicine mental health visits
Ensure greater access to culturally-competent primary care, dental, vision, and supportive services providers that are knowledgeable about HIV
- Develop HIV-competent provider network and list
- Develop relationships and provide training with new providers to expand the number of HIV-competent providers in our network
- Develop relationships with Hepatitis C and STI programs to integrate and strengthen testing, resources, and services when appropriate
Improve patient understanding of the health systems, treatment options, patient rights, and the tools they need to navigate their options and self-manage their care
- Increase community access to up-to-date, accurate medical information about HIV/Hep C/ STIs, as well as where to access treatment and supportive services
- Provide education and training on health systems and the health care landscape to all clients entering care with additional learning opportunities offered annually
1. 90% of people living with HIV in Louisiana will be retained in care
2. 90% of people living with HIV in care will be virally suppressed by 2025
- Ensure that all patients, providers, and the community at-large are aware of and understand U=U and how it impacts them
- Utilize peer support models to link all people who are newly diagnosed with HIV (and/or Hep C) with a peer mentor to help people get linked to care and to stay in care
- Ensure at least 80% of people who are newly diagnosed can start ARV meds within 7 days of diagnosis
- Increase transportation support for people living with HIV to access clinic appointments, support sessions, and pharmacy services throughout the state of Louisiana
- Reduce distance barriers and increase access to HIV care and treatment through the use of telemedicine and mobile health units
Improve access to services for all regardless of immigration status
- Use best practices to conduct outreach while building trust within community
- Offer testing and linkage to care through local consulates
- Assess existing policies and promote policies to ensure access to testing and treatment for all, regardless of immigration status
- Ensure Spanish-speaking staff and translators are available and located at facilities
We know that people living outside of our major cities face unique barriers to accessing care and services, maintaining confidentiality, and dealing with stigma and discrimination. While historically resources have been more limited in our rural communities, one of our goals is to center smaller cities and rural communities in our efforts to End the HIV Epidemic.
How are we getting loud?
We want to make sure that rural voices are heard and that their needs are prioritized. We want to raise awareness about how to prevent HIV and what it means to live with HIV (and what it doesn’t). We want to break down the misconceptions, fear, and stigma around HIV so that we can build community, capacity, and power across the state to improve the lives of those most impacted.
Work closely with organizations and key individuals who work directly with priority populations to raise awareness on HIV, STIs and Hep C
- Organize community outreach events tailored to specific groups (including but not limited to youth groups, young same-gender-loving African American men, African American women, people of transgender experience) with local partners and gatekeepers around the state
- Create agreements and improve referrals systems between HIV service agencies and primary health care centers, social services organizations to improve linkage to care for people diagnosed with HIV
Improve access to testing and treatment in rural areas by using new methods to reach people
- Increase use of mobile testing by expanding the Community Health Worker workforce and procuring and equipping additional mobile health units
- Expand testing at non-traditional sites through workplace wellness programs
- Provide options for home health visits through Ryan White funded agencies
- Offer in-home testing for HIV, STIs, and Hep C
- Expand use of telehealth for HIV and STI screening, treatment, case management, and to prescribe and manage PrEP
We believe that public health funding, resources, policy, and programs should be informed by both the data and the community. We need to improve data sharing and utilization, while maintaining and respecting confidentiality for our clients and residents. We have to measure what we don’t know, monitor our progress, and allocate funding and resources based on need. We must advocate for policies that both allow us to implement solutions that work for the community and allow us to reach our target outcomes.
How are we getting loud?
We want to go beyond ending the criminalization of HIV. We want to end the criminalization of poverty and vulnerable populations. In order to end stigma and the epidemics of HIV and Hep C, we need to put an end to discrimination based on race, sexuality, gender and gender identity, socio-economic status, immigration status, and HIV status. We recognize the lives of PLWH are often impacted by people not working in HIV, as such some of the strategies below seek to expand non-traditional stakeholder engagement.
Share data between agencies to identify clients who are not receiving care, and to improve linkage to care and treatment outcomes
- Use data to inform public health activities
- Expand Data-to-Care Programs to link patients to care (use pharmacy, Medicaid, Emergency Department, and Parish Jail data to better understand who is in need of services)
- Use data to evaluate where improvements are needed and work to increase the number of people who know their status, are in care, and who are virally suppressed
Reduce stigma, discrimination and criminalization of affected communities by advocating for policy changes at the statewide level and within institutions such as hospital systems, the Department of Corrections, the juvenile justice system, the foster care system, other social services, the courts, and universities
- Update HIV Criminal Statutes
- Work with policymakers and coalition partners to dra% and enact policies that build protection from discrimination into our laws (for PLWH, LGBTQ+ persons, immigrants)
- Integrate standards for equitable treatment of all people into all systems that PLWH and those at risk utilize to reduce criminalization by developing model policies and training staff on their responsibilities related to the American’s with Disabilities Act (ADA), cultural humility and anti-racism
- Conduct advocacy campaigns at the local and state level to raise awareness around HIV, HIV-related stigma and discrimination, and policies that intersect with the lives of PLWH and affected communities
- Create learning and training opportunities within universities and health professions to expand knowledge around HIV, STIs and Hep C for all providers and to train more Infectious Disease specialists
- Create learning and training opportunities for all providers of social services to reduce stigma and better understand the needs of those living with or vulnerable to HIV, including gender, sexual and ethnic minorities
Coordinate our response to ending the epidemic
- Maintain and grow our Statewide Planning Group through regular meetings and coalition-building
- Monitor, evaluate and share our progress with transparency through community-friendly platforms
We know that we have work to do, and we know we can’t do it alone. HIV has been a part of our lives for over four decades and though we make advances in treatment and prevention methods every day, systemic barriers continue to hold us back in our goals to ensure health and wellness for people living with HIV and to eliminate new transmissions. !e barriers we face can no longer be solved by science alone, or by the small but mighty community of advocates, providers, and public health workers in the HIV sphere, alone. We cannot eliminate poverty, house everyone experiencing homelessness, or rid our service providers of racism, homophobia and transphobia, alone. We cannot educate our entire populace about safer sex and testing, nor erase the stigma ingrained in their minds, alone.
As you can see, many of the strategies we have laid out depend on engaging others and finding allies across different spaces in our communities. We will need to expand our partnerships and work hand-in-hand with policymakers, educators, law enforcement, primary care and mental health providers, housing advocates, disability rights activists, faith leaders, community gatekeepers, and everyone in between.
Society at large still harbors too many harmful beliefs that keep PLWH living in fear and silence. We need those allies who feel safe in doing so, to break that silence and get loud by starting to talk to their friends and families – about sex, HIV, and STI prevention. Only then can we end the stigma that prevents people from ge”ing tested or seeking treatment, and isolates people from their support systems. Only then can we End the Epidemic.
So, as we move forward into implementing our plan, we are going to need you to come along… AND GET LOUD ABOUT IT!
 This plan would not have been possible without the hard work and creative energy of so many people. We, of course, want to thank the PLWH who continuously contribute to this work and whose expertise and willingness to share from their lived experience is invaluable. Countless stakeholders have contributed throughout this process—from Front Porch Talk participants and community advocates, to our public health workers at state and city agencies as well as community-based organizations across the state, to healthcare providers and community partners who have lent their knowledge and experience to strengthen our strategy.
This plan would not have been possible without the hard work and creative energy of so many people. We, of course, want to thank the PLWH who continuously contribute to this work and whose expertise and willingness to share from their lived experience is invaluable. Countless stakeholders have contributed throughout this process—from Front Porch Talk participants and community advocates, to our public health workers at state and city agencies as well as community-based organizations across the state, to healthcare providers and community partners who have lent their knowledge and experience to strengthen our strategy.
We also want to recognize those who we have lost during the creation of this plan, including two long term advocates that went above and beyond to give so much to our community, Chris Jackson and Gwen Guillory.
Access
Being able to have access to the resources needed to properly take care of one’s health
Ally
Someone who makes the commitment and effort to recognize their privilege (based on gender, class, race, sexual identity, etc.) and work in solidarity with oppressed groups in the struggle for justice. Allies understand that it is in their own interest to end all forms of oppression, even those from which they may benefit in concrete ways. Allies commit to reducing their own complicity or collusion in oppression of those groups and invest in strengthening their own knowledge and awareness of oppression.
AETC (AIDS Education and Training Center)
Regional centers providing education and training for primary care professionals and other AIDS-related personnel; authorized under Part F of the CARE Act and administered by HRSA’s Division of Training and Technical Assistance (DTTA)
AIDS (Acquired Immunodeficiency Syndrome)
Disease caused by the human immunodeficiency virus (HIV)
CBO (Community-Based Organization)
An organization that provides services to locally defined populations, which may or may not include populations diagnosed with or affected by HIV disease
Coalition
An alliance for collective action for a cause
Community
A group of people living in the same place or having a particular characteristic in common
Comprehensive Sex Education
According to the American College of Obstetricians and Gynecologists, comprehensive sexuality education should be “medically accurate, evidence-based, and age-appropriate, and should include the benefits of delaying sexual intercourse, while also providing information about normal reproductive development, contraception (including long-acting reversible contraception methods) to prevent unintended pregnancies, as well as barrier protection to prevent sexually transmitted infections (STIs).”
Continuum of Care
A coordinated delivery system, encompassing a comprehensive range of services needed by individuals or families with HIV infection, to meet their health care and psychosocial service needs throughout all stages of illness. !is is different from the HIV Care Continuum, which has a specific set of indicators.
Criminalization
Attempting to make someone seem like a criminal or wrongdoer by making their activities illegal or making it a point to associate their activities or features with negative traits or attributes
Epidemic
The spread of an infectious disease through a population or geographic area
Equity
The quality of being fair and impartial, and in a way that brings everyone to the same level versus giving everyone the same thing
FQHCs (Federally Qualified Health Centers)
Community-based health care providers that receive funds from the HRSA Health Center Program to provide primary care services in underserved areas
Gender Identity
A term used to describe the gender that an individual identifies with, which may or may not align with American gender binary roles outlined for their ascribed biological sex. It is a person’s sense of their own gender.
HBCUs
Historically Black Colleges and Universities
Health Disparity
Healthcare disparities refer to differences in access to or availability of facilities and services. Health status disparities refer to the variation in rates of disease occurrence and disabilities between socioeconomic and/or geographically defined population groups.
Health Literacy
The degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others
Holistic Health
Refers to caring for the whole person — providing for physical, mental, spiritual, and social needs
Human Rights
The basic and fundamental rights that should be given to all humans
Homophobia
Fear, anger, discomfort, intolerance, or lack of acceptance towards LGBTQ+ people, or experiencing these feelings about one’s own non-heterosexual orientation
Incarceration
The act of being confined in prison
Intersectionality
The idea that all oppressions are connected and should be addressed within the context of one another
LGBTQ+
“Lesbian, Gay, Bisexual, Transgender, Queer/Questioning” – May also be written as LGBTQI to include “Intersex” or LGBTQIA to include “Asexual”
Lived Experience
Personal knowledge of the world or an issue gained through direct, firsthand involvement rather than through secondary sources
Oppression
The economic, institutional and social and overall systemic ways in which a dominant group has mistreated, dis-serviced, and stigmatized subordinated groups of people
Outreach
The act of going out into a given community and using personal interactions to spread awareness and information
Person-Centered
Person- or patient-centered care, is defined by the World Health Organization as “empowering people to take charge of their own health rather than being passive recipients of services.”
Person-First Language
Language that puts the person first, such as using “person living with HIV” rather than “HIV patient”, or “person who injects drugs” instead of “drug addict”. It is also important to use the language preferred by the group being referred to and to use non-stigmatizing language.
Policy
A course or principle of action adopted or proposed by a government, party, business, or individual
Priority/Key Populations
Recognizable demographic subgroups of the general population, within which HIV/AIDS morbidity is comparatively high, increasing the risk of infection for others in the subgroup
PrEP (Pre-Exposure Prophylaxis)
A pill for people who do not have HIV and want added ongoing protection. It is available by prescription only, and must be taken every day – like birth control but for HIV prevention.
PEP (Post-Exposure Prophylaxis)
Another type of preventive medication intended for emergency situations only. PEP must be started within 72 hours a%er possible exposure to HIV. It also comes in pill form and requires a prescription.
PLWH
Person or people living with HIV disease
Racial Justice
The proactive reinforcement of policies, practices, attitudes and actions that produce equitable power, access, opportunities, treatment, impacts and outcomes for all
Racism
We use the term “racism” specifically to refer to individual, cultural, institutional and systemic ways by which differential consequences are created for groups historically or currently defined as white being advantaged, and groups historically or currently defined as non-white (African, Asian, Hispanic, Native American, etc.) as disadvantaged.
Re-entry
The process of formerly incarcerated people being given a fair chance to reintegrate with the world a%er being in prison
Reproductive Justice
An intersectional framework originally coined in 1994 by Black women as a concept that links reproductive rights with social justice. It is a response to the ways that mainstream feminist and reproductive rights movement did not account for the experiences of women of color who experience multiple forms of oppression. Sister Song defines RJ as the “right to not have children, right to have children, and the right to parent our children in safe and healthy environments.”
Reproductive Rights
The idea that women should not only have the ability to make choices for their bodies but access to the resources to do so
Ryan White HIV/AIDS Program
Health Resources and Services Administration’s (HRSA) program that provides a comprehensive system of HIV primary medical care, essential support services, and medications for low-income people living with HIV who are uninsured and underserved.
Safe Space
Spaces where people of a given marginalized group can find the comfort, safety, and support of others who understand and empathize or have lived the same experience. It is also a place where marginalized people can be unapologetically themselves without having to justify themselves to the oppressor.
Service Providers
Agencies/organizations which provide HIV services to patients/clients
Syringe Services Programs (SSPs)
Community-based HIV prevention strategy for persons who inject drugs (PWID). SSPs aim to reduce PWID’s risk of ge”ing and transmi”ing HIV, viral hepatitis, and other blood borne infections by using sterile injection equipment for each injection.
Stigma Index Project
The People Living with HIV Stigma Index provides a tool that measures and detects changing trends in relation to stigma and discrimination experienced by people living with HIV. In the initiative, the process is just as important as the product. It aims to address stigma relating to HIV while also advocating on the key barriers and issues perpetuating stigma —a key obstacle to HIV treatment, prevention, care and support.
Service
Resources that are given in exchange or for free to an individual or community that be”ers their quality of life
Social Justice
Fighting against unjust oppressive systems for the social, institutional, and economic wellbeing of marginalized people
Stigma
An attribute, behavior, or reputation which is socially discrediting in a particular way: it causes an individual to be mentally classified by others in an undesirable, rejected stereotype rather than in an accepted, normal one. HIV stigma refers to irrational or negative attitudes, behaviors, and judgments towards people living with or at risk of HIV.
Supportive Services
Services such as transportation, childcare, or dependent care, necessary to enable an individual to participate in activities, or other non-medical services to improve health and well-being such as mental health services, support groups, substance use supports, domestic violence services, housing services, etc.
Telehealth/TelePrEP
Telehealth the provision of healthcare remotely by means of telecommunications technology. TelePrEP is a program that allows you to virtually connect to a provider who can prescribe you PrEP through telemedicine. !is means you can use your personal electronic devices to have provider “visits” without having to leave your community.
Transgender or Trans*
An umbrella term for people whose gender identity is different from the sex they were assigned at birth
Transphobia
Refers to discrimination against transsexualism and transsexual or transgender people, based on the expression of their internal gender identity
Viral Suppression
When the amount of HIV in the body (viral load) reaches a very low level, which keeps the immune system working and prevents illness. !is is called viral suppression— the CDC defines this as having less than 200 copies of HIV per milliliter of blood. HIV medicine can even make the viral load so low that a test can’t detect it. This is called an undetectable viral load.
Wraparound Services
Non-medical case management, childcare, emergency financial assistance, food banks, housing services, substance use services, psychosocial support, and treatment adherence counseling
[1] National Health Care for the Homeless Council.
(2019, February). Homelessness and Health: What’s the Connection? Retrieved November 25, 2020, from
https://nhchc.org/wp-content/uploads/2019/08/homelessness-and-health.pdf
[2] Stotzer R. L. (2017).
Data Sources Hinder Our Understanding of Transgender Murders. American journal of public health, 107(9), 1362–1363.
https://doi.org/10.2105/AJPH.2017.303973
[3] PayScale. (2020).
Gender Pay Gap Statistics for 2020. Retrieved November 25, 2020, from
https://www.payscale.com/data/gender-pay-gap
[4] SisterSong, (n.d.).
Reproductive Justice. Retrieved November 25, 2020, from
https://www.sistersong.net/reproductive-justice
[5] The Sentencing Project.
(2020, July 28). State-by-State Data. Retrieved November 25, 2020, from
https://www.sentencingproject.org/the-facts/
[6] Cann, D., Harrison, S.E. & Qiao, S.
Historical and Current Trends in HIV Criminalization in South Carolina: Implications for the Southern HIV Epidemic. AIDS Behav 23, 233–241 (2019).
https://doi.org/10.1007/s10461-019-02599-1
[7] Intersectionality. (n.d.).
Retrieved November 25, 2020, from the link below. Originally coined by Kimberlé Crenshaw, 1989.
https://www.merriam-webster.com/dictionary/intersectionality
[8] Excerpted from the A Declaration of Liberation:
Building a Racially Just and Strategic Domestic HIV Movement by the Racial Justice Framework Group, a collaboration of the Positive Women’s Network and the CounterNarrative Project and their allies, accessed via
https://www.pwn-usa.org/old-policy-agenda/a-declaration-of-liberation-building-a-racially-just-and-strategic-domestic-hiv-movement/
[9] US Human Rights Network Human Core Principles, accessed via
https://www.ushrnetwork.org/about-us